Familial dysbetalipoproteinemia
 Print-Friendly
Print-Friendly
Type III hyperlipoproteinemia; Deficient or defective apolipoprotein E

Familial dysbetalipoproteinemia is a disorder passed down through families. It causes high amounts of cholesterol and triglycerides in the blood.
I Would Like to Learn About:
Causes
A genetic defect causes this condition. The defect results in the buildup of large lipoprotein particles that contain both cholesterol and a type of fat called triglycerides. The disease is linked to defects in the gene for apolipoprotein E.
Hypothyroidism, obesity, or diabetes can make the condition worse. Risk factors for familial dysbetalipoproteinemia include a family history of the disorder or coronary artery disease.
Symptoms
Symptoms may not be seen until age 20 or older.
Yellow deposits of fatty material in the skin called xanthomas may appear on the eyelids, palms of the hands, soles of the feet, or on the tendons of the ankles, knees and elbows.
Other symptoms may include:
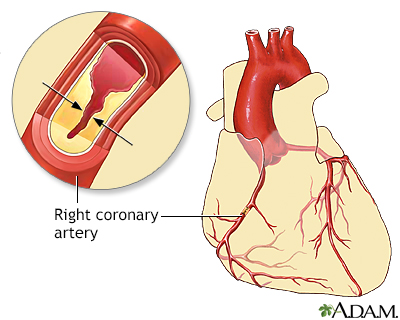
- Chest pain (angina) or other signs of coronary artery disease may be present at a young age
- Cramping of one or both calves when walking
- Sores on the toes that do not heal
- Sudden stroke-like symptoms such as trouble speaking, drooping on one side of the face, weakness of an arm or leg, and loss of balance
Exams and Tests
Tests that may be done to diagnose this condition include:
- Genetic testing for apolipoprotein E (apoE)
- Lipid panel blood test
- Triglyceride level
- Very low density lipoprotein (VLDL) test
Treatment
The goal of treatment is to control conditions such as obesity, hypothyroidism, and diabetes.
Making diet changes to reduce calories, saturated fats, and cholesterol may help lower blood cholesterol.
If cholesterol and triglyceride levels are still high after you have made diet changes, your health care provider may have you take medicines as well. Medicines to lower blood triglyceride and cholesterol levels include:
- Bile acid-sequestering resins.
- Fibrates (gemfibrozil, fenofibrate).
- Nicotinic acid.
- Statins.
- PCSK9 inhibitors, such as alirocumab (Praluent) and evolocumab (Repatha). These represent a newer class of drugs to treat cholesterol.
Outlook (Prognosis)
People with this condition have a significantly increased risk for coronary artery disease and peripheral vascular disease.
With treatment, most people are able to greatly reduce their levels of cholesterol and triglycerides.
Possible Complications
Complications may include:
- Heart attack
- Stroke
- Peripheral vascular disease
- Intermittent claudication
- Gangrene of the lower extremities
When to Contact a Medical Professional
Contact your provider if you have been diagnosed with this disorder and:
- New symptoms develop.
- Symptoms do not improve with treatment.
- Symptoms get worse.
Prevention
Screening the family members of people with this condition may lead to early detection and treatment.
Getting treated early and limiting other risk factors such as smoking can help prevent early heart attacks, strokes, and blocked blood vessels.









Related Information
| AtherosclerosisStable anginaPeripheral artery ...HypothyroidismOverweightDiabetesHeart attack | Cholesterol - InDe...Coronary artery di...Peripheral artery ... |
References
Genest J, Mora S, Libby P. Lipoprotein disorders and cardiovascular disease. In: Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, Solomon SD, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Philadelphia, PA: Elsevier; 2022:chap 27.
Robinson JG. Disorders of lipid metabolism. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 26th ed. Philadelphia, PA: Elsevier; 2020:chap 195.