
Shunt - ventriculoperitoneal; VP shunt; Shunt revision
Ventriculoperitoneal shunting is surgery to treat excess cerebrospinal fluid (CSF) in the cavities (ventricles) of the brain (hydrocephalus).
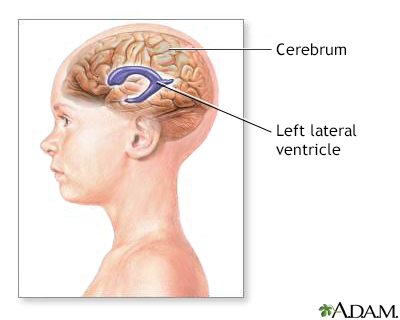
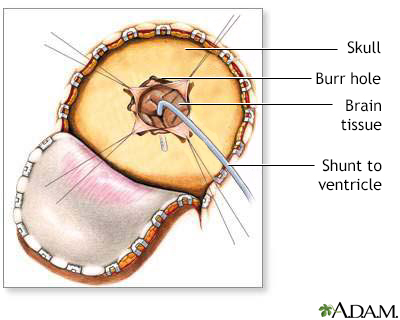
This procedure is done in the operating room under general anesthesia. It takes about 1 1/2 hours. A thin tube (catheter) is passed from the cavities of the head to the abdomen to drain the excess CSF. A pressure valve and an anti-siphon device ensure that just the right amount of fluid is drained.
The procedure is done as follows:
This surgery is done when there is too much CSF in the brain and spinal cord. This is called hydrocephalus. It causes higher than normal pressure on the brain. It can cause brain damage.
Children may be born with hydrocephalus. It can occur with other birth defects of the spinal column or brain. Hydrocephalus can also occur in older adults.
Shunt surgery should be done as soon as hydrocephalus is diagnosed. Alternative surgeries may be proposed. Your doctor can tell you more about these options.
Risks of anesthesia and surgery in general are:
Risks of ventriculoperitoneal shunt placement are:
The shunt may stop working. If this happens, fluid will begin to build up in the brain again. As a child grows, the shunt may need to be repositioned.
Tell your surgeon or nurse if:
Planning for your surgery:
During the week before your surgery:
On the day of surgery:
The person may need to lie flat for 24 hours the first time a shunt is placed.
How long the hospital stay is depends on the reason the shunt is needed. The health care team will closely monitor the person. Intravenous (IV) fluids, antibiotics, and pain medicines will be given if needed.
Follow the surgeon's instructions about how to take care of the shunt at home. This may include taking medicine to prevent infection of the shunt.
Shunt placement is usually successful in reducing pressure in the brain. But if hydrocephalus is related to other conditions, such as spina bifida, brain tumor, meningitis, encephalitis, or hemorrhage, these conditions could affect the prognosis. How severe hydrocephalus is before surgery also affects the outcome.
Badhiwala JH, Kulkarni AV. Ventricular shunting procedures. In: Winn HR, ed. Youmans and Winn Neurological Surgery. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 227.
Rosenberg GA. Brain edema and disorders of cerebrospinal fluid circulation. In: Jankovic J, Mazziotta JC, Pomeroy SL, Newman NJ, eds. Bradley and Daroff's Neurology in Clinical Practice. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 88.
BACK TO TOPReview Date: 12/31/2023
Reviewed By: Joseph V. Campellone, MD, Department of Neurology, Cooper Medical School at Rowan University, Camden, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.

|
A.D.A.M., Inc. is accredited by URAC, also known as the American Accreditation HealthCare Commission (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics and subscribes to the principles of the Health on the Net Foundation (www.hon.ch). |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Call 911 for all medical emergencies. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. © 1997- A.D.A.M., Inc. Any duplication or distribution of the information contained herein is strictly prohibited.